
Preprint EDGE K NOWLEDGE -DRIVEN NEW DRUG RECOM - MENDATION
2025-05-02
1
0
912.75KB
17 页
10玖币
侵权投诉

Preprint
EDGE: KNOWLEDGE-DRIVEN NEW DRUG RECOM-
MENDATION
Zhenbang Wu1, Huaxiu Yao2, Zhe Su3, David M Liebovitz4, Lucas M Glass5,
James Zou2, Chelsea Finn2, Jimeng Sun1
ABSTRACT
Drug recommendation assists doctors in prescribing personalized medications to
patients based on their health conditions. Existing drug recommendation solutions
adopt the supervised multi-label classification setup and only work with existing
drugs with sufficient prescription data from many patients. However, newly ap-
proved drugs do not have much historical prescription data and cannot leverage
existing drug recommendation methods. To address this, we formulate the new
drug recommendation as a few-shot learning problem. Yet, directly applying ex-
isting few-shot learning algorithms faces two challenges: (1) complex relations
among diseases and drugs and (2) numerous false-negative patients who were
eligible but did not yet use the new drugs. To tackle these challenges, we pro-
pose EDGE, which can quickly adapt to the recommendation for a new drug with
limited prescription data from a few support patients. EDGE maintains a drug-
dependent multi-phenotype few-shot learner to bridge the gap between existing
and new drugs. Specifically, EDGE leverages the drug ontology to link new drugs
to existing drugs with similar treatment effects and learns ontology-based drug
representations. Such drug representations are used to customize the metric space
of the phenotype-driven patient representations, which are composed of a set of
phenotypes capturing complex patient health status. Lastly, EDGE eliminates the
false-negative supervision signal using an external drug-disease knowledge base.
We evaluate EDGE on two real-world datasets: the public EHR data (MIMIC-
IV) and private industrial claims data. Results show that EDGE achieves 7.3%
improvement on the ROC-AUC score over the best baseline.
1 INTRODUCTION
With the wide adoption of electronic health records (EHR) and the advance of deep learning models,
we have seen great opportunities in assisting clinical decisions with deep learning models to improve
resource utilization, healthcare quality, and patient safety (Xiao et al., 2018). Drug recommendation
is one of the essential applications which aims at assisting doctors in recommending personalized
medications to patients based on their health conditions. Existing drug recommendation methods
typically formulate it as a supervised multi-label classification problem (Zhang et al., 2017; Zitnik
et al., 2018; Shang et al., 2019b; Yang et al., 2021; Wu et al., 2022; Tan et al., 2022b). They often
train on massive prescription data to learn patient representations and use the learned representations
to predict medications (i.e., labels). However, in reality, new drugs come to the market all the time.
For example, U.S. Food and Drug Administration (FDA) approves a wide range of new drugs every
year (FDA, 2022). Most of these newly approved drugs do not have much historical data to support
model training (Blass, 2021). Even if sufficient prescription data for new drugs exists, existing
models must be periodically re-trained or updated to recommend new drugs, which is expensive and
complex. As a result, existing drug recommendation methods can only recommend the same set of
drugs seen during training and are no longer applicable when new drugs appear.
To address this, we formulate the recommendation of new drugs as a few-shot classification problem.
Given a new drug with limited prescription data from a few support patients (e.g., from clinical
trials (Duijnhoven et al., 2013)), the model should quickly adapt to the recommendation for this drug.
1University of Illinois Urbana-Champaign, 2Stanford University, 3Zhejiang University, 4Northwestern
University, 5IQVIA, Corresponding authors: zw12@illinois.edu
1
arXiv:2210.05572v1 [cs.LG] 11 Oct 2022

Preprint
Meta-learning approaches have been widely used in such problems by learning how to quickly adapt
the classifier to a new label unseen during training, given only a few support examples (Finn et al.,
2017; Snell et al., 2017). However, most prior meta-learning works focus on vision or language-
related tasks. In the new drug recommendation, applying existing meta-learning algorithms faces the
following challenges. (1) Complex relations among diseases and drugs: diseases and medicines
can have inherent and higher order relations. Deciding whether to prescribe a drug to a specific
patient depends on many factors, such as disease progression, comorbidities, ongoing treatments,
individual drug response, and drug side effects. General meta-learning algorithms do not explicitly
capture such dependencies. (2) Numerous false-negative patients: many drugs can treat the same
disease, but usually, only one of them is prescribed. For any given drug, there exist many false-
negative patients who were eligible but did not yet use the new drug (e.g., due to drug availability,
doctor’s preference, or insurance coverage). The number of false-negative supervision signals will
substantially confuse the model learning, especially in the few-shot learning setting.
To address these challenges, we introduce EDGE, a drug-dependent multi-phenotype few-shot
learner to quickly adapt to the recommendation for a new drug with limited support patients. Specif-
ically, since drugs within the same category often have similar treatment effects, EDGE utilizes the
drug ontology for drug representation learning to link new drugs with existing drugs. Further, EDGE
learns multi-phenotype patient representations to capture the complex patient health status from dif-
ferent aspects such as chronic diseases, current symptoms, and ongoing treatments. Given a new
drug with a few support patients, EDGE makes recommendations by performing a drug-dependent
phenotype-level comparison between representations of query patients and corresponding support
prototypes. Lastly, to reduce the false-negative supervision signal, EDGE leverages the MEDI (Wei
et al., 2013) drug-disease knowledge base to guide the negative sampling process.
The main contributions of this work include:
• To our best knowledge, this is the first work formulating the task of new drug recommendation;
• We propose a meta-learning framework EDGE to solve this problem by considering complicated
relations among diseases and drugs, and eliminating numerous false-negative patients.
• We conduct extensive experiments on the public EHR data MIMIC-IV (Johnson et al., 2020)
and private industrial claims data. Results show that our approach achieves 5.6% over ROC-AUC,
6.3% over Precision@100, and 5.5% over Recall@100 when providing recommended patient lists
for new drugs. We also include detailed analyses and ablation studies to show the effectiveness of
multi-phenotype patient representation, drug-dependent patient distance, and knowledge-guided
negative sampling.
2 PROBLEM FORMULATION AND PRELIMINARIES
Denote the set of all drugs as M; the goal of drug recommendation is to prescribe drugs in M
that are suitable for a patient with a record v= [c1, . . . , cV], which consists of a list of diseases
(and procedures), and Vis the total number of diseases and procedures in the record v. Prior
works (Zhang et al., 2017; Shang et al., 2019b; Yang et al., 2021; Tan et al., 2022b) formulate drug
recommendation as a multi-label classification problem by generating a multi-hot output of size
|M|. However, this formulation assumes that the drug label space Mremains unchanged after
training and is not applicable when new drugs appear. Thus, we propose an alternative formulation
for the new drug recommendation as follows.
Assume the entire drug set Mis partitioned into a set of existing drugs Mold and a set of new
drugs Mnew, where Mold ∩ Mnew =∅. Each existing drug mi∈ Mold has sufficient patients
using the drug mi(e.g., from EHR data). Each new drug mt∈ Mnew is associated with a small
support set St={vj}Ns
j=1 consisting of patients using the drug mt(e.g., from clinical trials), and
an unlabeled query patient set Qt={vj}Nq
j=1, where Nsand Nqare the number of patients in the
support and query sets, respectively. The goal of new drug recommendation is to train a model fφ(·)
parameterized by φon existing drugs Mold, such that it can adapt to new drug mt∈ Mnew given
the small support set St, and make correct recommendation on the query set Qt.
To reduce clutter, we use a unified notation for both diseases and procedures. Since we focus on record-
level prediction, “patient” and “record” are used interchangeably.
2

Preprint
𝑓
$!
%!
𝑐"𝑐#𝑐$𝑐%𝑐&
%"%$%#%%
&
'!&
'!&
'!
𝐠'() 𝐠'*) 𝐠'+)
𝐡
𝐦"
𝐦#
𝐦$
𝛼!,#
𝛼!,"
𝛼!,!
Ontology-Enhanced
Drug Representation
Multi-Phenotype
Patient Representation Drug-Dependent Patient Distance
Query
𝒢(")
,
,,
,
,-
-
-
-
-
.$
."
.!
&
'"
𝐡
Σ
𝐩(!)
𝐩#(%)
𝑣*
𝑧(%)
𝑧#(%)
𝐠*
(!)
Medication Disease Procedure Patient Record Phenotype ,
-Pos/Neg Support
Figure 1: EDGE learns the ontology-enhanced drug representation hand multi-phenotype patient
representations {g(l)}3
l=1. For a new drug m1,EDGE decides whether to prescribe it to a query
patient vqby performing a drug-dependent phenotype-level comparison between multi-phenotype
query representations {g(l)
q}3
l=1 and corresponding support prototypes {p(l)}3
l=1.
Our work is inspired by the prototypical network (Snell et al., 2017), which learns a representation
model fφ(·)such that patients using a specific drug will cluster around a prototype representation.
Recommendation can then be performed by computing the distance to the prototype. To equip the
model with the ability to adapt to new drug with limited support patients, prototypical network
trains the model via episodic training, where each episode is designed to mimic the low-data testing
regime. Concretely, an episode is formed by first sampling an existing drug mifrom Mold and then
sampling a set of patients using the drug mi. The sampled patients are divided into two disjoint sets:
(1) a support set Siused to calculate the prototype, and (2) a query set Qiused to calculate the loss.
From the support set Si, prototypical network calculates the prototype representation as,
p=1
|Si|X
j∈Si
fφ(vj),p∈Re,(1)
where pis an e-dimensional vector in the metric space, and |·|denotes cardinality. Next, given a
query patient vq, the probability of recommending drug miis measured by the distance d(·)between
its representation and the corresponding prototypes as,
pφ(yq= +|vq) = exp (−d(fφ(vq),p))
exp (−d(fφ(vq),p)) + exp (−d(fφ(vq),p0)) ,(2)
where p0is the negative prototype obtained from another negative support set S0
iof patients not using
the drug mi(i.e., negative sampling). The loss is computed as the negative log-likelihood (NLL)
loss L(φ) = −log pφ(yq=∗|vq)of the true label ∗∈{+,−}. And the model fφ(·)is optimized on
both the query set Qiand another negative query set Q0
iobtained via negative sampling (similarly
as S0
i).
3 KNOWLEDGE-DRIVEN NEW DRUG RECOMMENDATION
In this section, we introduce EDGE, which can adapt to new drugs with limited support patients via
a drug-dependent multi-phenotype few-shot learner. Specifically, EDGE consists of the following
modules: (1) Ontology-enhanced drug encoder that fuses ontology information into drug repre-
sentation to link new drugs to existing drugs with similar treatment effects; (2) Multi-phenotype
patient encoder that represents each patient with a set of phenotype-level representations to cap-
ture the complex patient’s health status; (3) Drug-dependent distance measures that learns drug-
dependent phenotype importance scores to customize the patient similarity; (4) knowledge-guide
negative sampling that eliminates the false-negative supervision signal. Figure 1 provides an illus-
tration of EDGE. In the following, we will describe how EDGE decides whether to prescribe a drug
mito a query patient vq, given a small set of support patients Siusing the drug mi.
3.1 ONTOLOGY-ENHANCED DRUG REPRESENTATION LEARNING
Though many new drugs have not been used regularly in clinical practice, they still belong to the
same drug category (from a drug ontology) as some existing drugs and share similar treatment ef-
fects, implicitly indicating similar patient populations. For example, the newly approved Quviviq
3

Preprint
for treating insomnia belongs to the same category (Orexin Receptor Antagonist) as some existing
drugs, like Belsomra and Dayvigo, which are also sleeping aids. We here leverage the drug ontol-
ogy to enrich the drug representation by attentively combing the drug itself and its corresponding
ancestors (e.g., higher-level drug categories).
Concretely, for the drug mi, we obtain its basic embeddings mi∈Reby feeding its description
into Clinical-BERT (Alsentzer et al., 2019). Then, follow Choi et al. (2017), we use the basic
embeddings of drug miand its ancestors to calculate the ontology-enriched drug representation as,
h=X
j∈Ai
αi,j mj,h∈Re,(3)
where Aidenotes the set of drug miand its ancestors, and the attention score αi,j represents the
importance of ancestor mjfor drug mi, which is calculated as,
αi,j =exp(fφa(mi⊕mj))
Pk∈Aiexp(fφa(mi⊕mk)) , αi,j ∈[0,1],(4)
where ⊕denotes the concatenation operator, and fφa(·) : R2e7→ Ris defined as a two-layer fully
connected neural network with Tanh activation. In this way, we fuse the ontology information into
the representation hfor drug mi, which is later used to customize the metric space of phenotype-
driven patient representations, introduced next.
3.2 MULTI-PHENOTYPE PATIENT REPRESENTATION LEARNING
Patient health status includes many factors, such as disease progression, comorbidities, ongoing
treatments, individual drug response, and drug side effects. Encoding each patient into a single
vector may not capture the complete information, especially for patients with complex health con-
ditions. Therefore, we define a set of phenotypes and represent each patient with a set of phenotype
vectors. Each phenotype can provide helpful guidance in patient representation learning and further
benefit the new drug recommendation.
Specifically, for every support/query patient vwith a list of diseases [c1, . . . , cV],EDGE first com-
putes the contextualized disease representations by applying the embedding function fφr(·)as,
[r1,...,rV] = fφr([c1,...,cV]) ,rj∈Re,(5)
where rjis the contextualized representation for disease cj. We model fφr(·)using a bi-directional
gated recurrent unit (GRU) due to its popularity in prior works (Zhang et al., 2017; Shang et al.,
2019b; Yang et al., 2021), and also show results with multilayer perceptron (MLP) and Trans-
former (Vaswani et al., 2017) in our experiments.
Next, we leverage domain knowledge to group diseases into different phenotypes. To obtain the
representation for the l-th phenotype, we take the representations from all diseases that belong to
that phenotype, project them to a lower dimension, and calculate their mean representations as,
g(l)=1
|G(l)|X
j∈G(l)
fφg(rj),g(l)∈Rg,(6)
where G(l)represents the set of diseases whose phenotype is l, and fφg(·) : Re→Rgis single-layer
neural network and g < e. We show results with different values of gin the experiment. If G(l)
is empty, we take the pooled sequence representation as a substitute. The phenotypes are extracted
from Clinical Classification Software (CCS) (H. CUP, 2010). There are 511 phenotypes in total. In
this way, each support/query patient is represented with a set of phenotype vectors {g(l)}L
l=1.
Based on the multi-phenotype patient representations, we further calculate the phenotype-level pro-
totypes from the support set Siof drug mi, where equation 1 is revised as,
p(l)=1
|Si|X
j∈Si
g(l)
j,p(l)∈Rg,(7)
E.g., Ibuprofen is a nonsteroidal anti-inflammatory drug that is used for treating pain, fever, and inflam-
mation.
4

摘要:
展开>>
收起<<
PreprintEDGE:KNOWLEDGE-DRIVENNEWDRUGRECOM-MENDATIONZhenbangWu1,HuaxiuYao2,ZheSu3,DavidMLiebovitz4,LucasMGlass5,JamesZou2,ChelseaFinn2,JimengSun1ABSTRACTDrugrecommendationassistsdoctorsinprescribingpersonalizedmedicationstopatientsbasedontheirhealthconditions.Existingdrugrecommendationsolutionsadoptt...
声明:本站为文档C2C交易模式,即用户上传的文档直接被用户下载,本站只是中间服务平台,本站所有文档下载所得的收益归上传人(含作者)所有。玖贝云文库仅提供信息存储空间,仅对用户上传内容的表现方式做保护处理,对上载内容本身不做任何修改或编辑。若文档所含内容侵犯了您的版权或隐私,请立即通知玖贝云文库,我们立即给予删除!
相关推荐
-
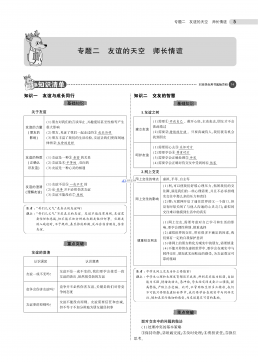
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包05专题五 走进社会生活 遵守社会规则VIP免费
 2024-11-21 24
2024-11-21 24 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包05专题五 走进社会生活 遵守社会规则VIP免费
 2024-11-21 24
2024-11-21 24 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包03专题三 青春时光 做情绪情感的主人VIP免费
 2024-11-21 16
2024-11-21 16 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包03专题三 青春时光 做情绪情感的主人VIP免费
 2024-11-21 22
2024-11-21 22 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包02专题二 友谊的天空 师长情谊VIP免费
 2024-11-21 19
2024-11-21 19 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包02专题二 友谊的天空 师长情谊VIP免费
 2024-11-21 20
2024-11-21 20 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包01专题一 成长的节拍 生命的思考VIP免费
 2024-11-21 25
2024-11-21 25 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包01专题一 成长的节拍 生命的思考VIP免费
 2024-11-21 24
2024-11-21 24 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包《53中考》全国道德与法治资料包VIP免费
 2024-11-21 27
2024-11-21 27 -
曲一线系列初中《5中考3年模拟》2023专题解释全国道德与法治资料包07专题七 坚持宪法至上 崇尚法治精神VIP免费
 2024-11-21 19
2024-11-21 19
分类:图书资源
价格:10玖币
属性:17 页
大小:912.75KB
格式:PDF
时间:2025-05-02
作者详情


相关内容
-
2025届重庆市西南大学附属中学高三下学期5月全镇模拟物理试题(含答案)
分类:中学教育
时间:2025-12-31
标签:无
格式:PDF
价格:10 玖币
-
2025届重庆市西南大学附属中学高三下学期5月全镇模拟化学试题(含答案)
分类:中学教育
时间:2025-12-31
标签:无
格式:PDF
价格:10 玖币
-
2025届浙江省新阵地联盟高三10月联考数学答案
分类:中学教育
时间:2025-12-31
标签:无
格式:PDF
价格:10 玖币
-

2025届重庆市西南大学附属中学高三下学期5月全镇模拟数学试题(含答案)
分类:中学教育
时间:2025-12-31
标签:无
格式:PDF
价格:10 玖币
-
2025届重庆康德三诊英语+答案
分类:中学教育
时间:2026-01-03
标签:无
格式:PDF
价格:10 玖币

